Fatty Liver Disease
In today’s fast-paced world, our lifestyles have undergone significant changes, impacting our health in ways we might not even realize. One such health concern that has been on the rise is Fatty Liver Disease, or steatosis. Let’s delve into this topic to gain a deeper understanding of its nuances and implications.
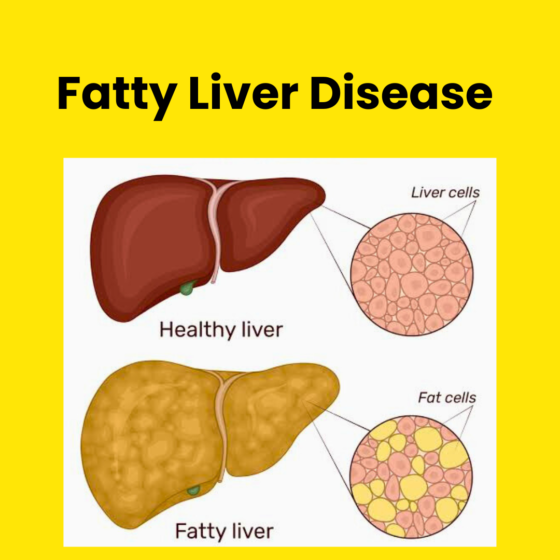
What is Fatty Liver Disease?
Fatty liver disease occurs when an excess amount of fat accumulates within the liver. While a certain level of fat is normal, the concern arises when it reaches 5-10% of the liver’s weight. At the early stages, this might not manifest with severe symptoms, but if left unchecked, it can progress and lead to more severe complications.
🔴 The Stages of Progression
1️⃣ Steatohepatitis: The liver becomes inflamed and swollen, causing damage to its tissue.
2️⃣ Fibrosis: Scar tissue develops in response to ongoing liver damage.
3️⃣ Cirrhosis: Extensive scar tissue replaces healthy liver tissue, hindering its proper functioning. Cirrhosis can have dire consequences, including liver failure and a heightened risk of liver cancer.
🥃 Alcohol-induced vs. Non-alcohol Related
There are two primary forms of fatty liver disease: alcohol-induced and non-alcohol related. Alcohol-induced fatty liver disease is linked to excessive alcohol consumption and affects approximately 5% of people in the India 🇮🇳 . On the other hand, non-alcohol related fatty liver disease (NAFLD) affects a staggering 1 in 3 adults in India. While the exact causes of NAFLD aren’t fully understood, factors such as obesity and diabetes appear to play a significant role.
🎯 Identifying Risk Factors
Certain factors can increase your susceptibility to developing fatty liver disease:
✅ Genetics
✅ Ethnicity: Individuals of Hispanic or Asian descent are at a higher risk.
✅ Menopause: Completed menopause can impact vulnerability.
✅ Obesity and Abdominal Fat: Excess belly fat is a red flag.
✅ Metabolic Factors: Conditions like high blood pressure, diabetes, and high cholesterol.
✅ Sleep Apnea: Obstructive sleep apnea can contribute to the condition.
Knowledge is power, and understanding fatty liver disease empowers us to make informed choices for our health. Prioritizing liver health through mindful lifestyle choices, regular exercise, and a balanced diet can go a long way in prevention and management.
Let’s spread awareness and work together towards better liver health! #healthawareness #fattyliver